Primary care serves as the foundation of a well-functioning healthcare system. It can point patients in the right direction to improve their health status, manage existing conditions, and spot problems before they become serious. Across the country, more than 35% of healthcare visits are provided by primary care, yet it receives only 5% of health spending[1]. As a result of this underfunding, there are long wait times to see a primary care provider and missed opportunities to manage preventable disease exacerbations. There is a more efficient and effective way to spend our health care dollars by better resourcing primary care and there is a national movement afoot to bolster primary care.
Robust, widely available primary care is needed more than ever in Michigan. Even now, 25% of Michiganders lack a usual source of care. Looming losses in Medicaid coverage from the One Big Beautiful Bill Act (OBBA) and escalating premiums place an even greater strain on primary care. In addition to Michigan’s affordability and access challenges, the population of the state is growing sicker. Rates of frequent physical distress, low birth weight, multiple chronic conditions and obesity rates in Michigan now exceed the national average[2]. Of Michigan’s 83 counties, over 70 are designated by the Health Resources and Services Administration (HRSA) as Health Professional Shortage Areas (HPSAs), areas with more than 3,500 people for every one primary care provider.
There is good evidence that robust, evidence-based primary care is cost-effective and improves population health, reducing the burden of chronic disease, lowering healthcare costs, and delivering patient satisfaction.[3] Areas with higher ratios of primary care physicians to population have lower costs of care and better health outcomes.[4] The strength of the evidence supporting the important role of accessible, effective primary care for patients has catalyzed action across the nation. More than a third of states have already passed legislation or enacted regulation to increase the percentage of spending that goes to primary care.
The National Academies of Science, Engineering, and Medicine (NASEM) 2021 report on Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care[5] provides a robust set of principles and recommendations for improving primary care. It emphasizes an integrated, whole-person health model of care that is delivered by an interprofessional team that partners with patients. This interprofessional team is comprised of a primary care physician who leads a team of health care professionals (e.g., NP/PAs, RN Care Managers, other nurses, medical assistants, and additional ancillary staff such as social workers, community health workers, and pharmacists, etc.) that focus on each patient’s health needs to design a patient care plan.
The Center for Medicare and Medicaid Innovation’s (CMMI’s) AHEAD demonstration is a federal model that increases investment in primary care as a part of a larger strategy to curb growth in overall health care costs, provide financial stability for hospitals, and support beneficiary connection to community resources. Six states (Maryland, Connecticut, Hawaii, Vermont, Rhode Island, and New York) participate in AHEAD so far. The model requires participation of the State, and a set of hospital partners. Thus far in Michigan, there has not been interest from the state or hospital partners in participating in AHEAD.
More than 20 states have taken action to increase investment in primary care, including some of the AHEAD states mentioned above. The way that states elect to define primary care spending varies, but for context, the latest version of the Primary Care Spending Dashboards released by the Milbank Fund show Michigan spending across all payer types for the narrow definition of primary care (i.e., payment to primary care physicians) at 5.5%.
Among the states that have passed legislation to increase investment in primary care are:
- California’s Health Care Affordability Board approved two related primary care investment benchmarks in October 2024: 1) a statewide investment benchmark of 15% of total medical expense (TME) allocated to primary care for all payers by 2034; and 2) an annual improvement benchmark of 0.5-1 percentage point per year increase in primary care spending as a share of TME for each payer for years 2025-2033. The Office of Health Care Affordability (OHCA) measures and reports on primary care investment, with the first public reporting scheduled for 2026. Though the benchmark is not enforceable, the hope is that plans will voluntarily meet targets. California also has a statewide health care spending target, set at 3.5% for 2025 and phasing down to 3.0% for 2029, which is enforceable.[6]. In addition, the state’s Medicaid program, Medi-Cal, increased rates for primary care services to 87.5% of Medicare rates, effective January 1, 2024.
- Delaware has set a primary care target of 11.5% of total medical spending by 2025 for private insurers and a requirement to match Medicare reimbursement rates for primary care[7]. However, a recent Delaware Primary Care Reform Collaborative strategic plan report[8] expressed concern about the extent to which Medicaid and commercial payers are meeting their expectations. Members of the state’s Primary Care Reform Collaborative noted at their August 2025 meeting that the state is exploring participation in the federal AHEAD model as a promising long-term option.
- Oregon’s strategy to increase primary care has been perhaps the nation’s most successful over time. In 2015, the state created the Primary Care Payment Reform Collaborative to study primary care spending and issue recommendations. State Bill 934 in 2017 required Oregon’s Coordinated Care Organizations and plans for public employees and educators to spend at least 12% of their total budget on primary care by January 2023. The state has impressive public-facing Oregon Primary Care Spending Dashboards that report the overall primary care spending rate for primary care at or above 13% of total medical spending for all lines of business (e.g., commercial, Medicaid, Medicare Advantage). The Oregon report cards show not only primary care spending as a percentage of total spending by plan type, but also the extent of non-claims spending on primary care and primary care spending by plan. Oregon also has a cost growth target program that sets a 3.4% cap on cost growth for most payers. The overall cost growth targets ensures that increased investment in primary care will not be inflationary.
- Oklahoma focuses its primary care investment actions on Medicaid spending. SB 563 directs the Oklahoma Health Care Authority to transition Medicaid from FFS to managed care and requires that 11% of spending to be spent on primary care by its Medicaid managed care organizations (MCOs) no later than the fourth year of a contract with the Medicaid program.
- Rhode Island was the first state to adopt policies to increase primary care spending through its 2010 affordability standards, requiring commercial insurers to increase the share of health care spending allocated to primary care by 1% annually, while hospital price growth was capped at the Medicare price index plus 1%. The state required corrective action plans for meeting the primary care investment targets and included an enforcement mechanism to motivate improvement. Primary care spending subsequently increased, while total spending slowed, driven by hospital price growth caps. By 2018, 12.3% of spending by commercial insurers went to primary care, though upon further exploration the state found that the definition of primary care spending was overly broad and revised the definition to be narrower to address the root challenges for primary care. The new, narrower definition became effective beginning September 2024 and is set at a 10% target primary care spending of total medical spending.[9]
- Washington State’s primary care investment target, set by legislation (SB 5589), is set at reaching 12% of total healthcare spending on primary care. An advisory committee is working to define measures, track progress, and recommend strategies for payers (insurers, state plans) to meet this goal, aiming to shift away from fee-for-service towards team-based care. Current spending is significantly lower (around 6%), highlighting the need for increased investment, with some suggesting annual increases of 1-2%. The target is not enforceable and does not have a statutory enforcement mechanism (such as financial penalties or fines for non-compliance) for payers that fail to meet the goal. Instead, the state relies on voluntary measures, public reporting, and monitoring through the Health Care Cost Transparency Board.
Among the states with bills introduced or other proposed state actions to increase investment in primary care:
- Colorado’s HB19-1233 established a Primary Care Payment Reform Collaborative that started meeting in July 2019 and has been extended until 2032. The Collaborative’s work includes measuring the percent of medical spending by plan. The legislation also requires commercial insurers to increase primary care spending by 1% in 2022 and another percent in 2023 and insurers are prohibited from raising premiums to cover the increased spending on primary care. The Collaborative uses Center for Improving Value in Health Care (CIVHC) Colorado data to track changes in primary care investment over time. They found that primary care spending across all reporting payer types has increased from 14.8% in 2022 to 15.7% in 2024, though it is uneven among payer types.
- In 2021, Hawaii required Medicaid Managed Care Organizations (MCOs) to report on and increase the percentage of medical expenditure devoted to primary care. This did not result in increased primary care spending due to pandemic-driven pressures and other challenges. However, Hawaii is an AHEAD state and this will increase primary care funding for participating practices. In addition, Hawaii’s SB1646 introduced in 2025 requires the Hawaii Employer-Union Health Benefits Trust Fund Board of Trustees to negotiate with health insurance carriers to ensure that 12% of monthly premium payments are paid directly to primary care providers.
- In the fall of 2007, the Maine Legislature convened the Commission to Study Primary Care Practice to examine the issues facing primary care and ways to stabilize and support it. In the 2008-2009 State Health Plan, the Governor’s Office for Health Policy and Finance identified the need to promote primary care as the foundation for the state’s health system. The Maine Quality Forum issues annual reports, pursuant to Public Law 2019, Chapter 244. The most recent (November 20, 2025) report found that in the most recent year of reporting, 2023, primary care spending as a percentage of total payments was highest for MaineCare (11.6-12.7%), followed by Medicare (9.6%) and commercial payors (7.6%).
- Maryland has a history of success in supporting primary care practices often paired with or as a part of larger reform efforts. For example, the state entered into a Total Cost of Care Model with the Federal Government designed to coordinate care for patients across both hospital and non-hospital settings, improve health outcomes, and constrain the growth of health care costs. A key element of the model was the Maryland Primary Care Program (MDPCP), a voluntary program open to all qualifying Maryland primary care providers that provides funding and support for the delivery of advanced primary care throughout the state. The model is comprehensive and offers pharmacist, health and nutrition counseling, behavioral health, coordinated referrals and linkages to social services and support from health educators and community health workers to provide an integrated experience for patients. The state uses Care Transformation Organizations (CTOs) to allow practices to avail themselves of these resources without the need for direct investment. Public reporting has demonstrated that the MDPCP has contributed to decreases in Medicare total expenditures, as well as decreases in inpatient and emergency room utilization, all while maintaining budget neutrality. In addition to the MDPCP, Maryland will begin its implementation of AHEAD in January 2026 at which point MDPCP will become part of AHEAD in Maryland.
- In December of 2025, the Massachusetts Primary Care Access, Delivery, and Payment Task Force released its first report, which recommended that a target for spending on primary care in Massachusetts be set at 15% of total healthcare spending, or double the current primary care spending share, whichever is greater, within five years of 2026. The Massachusetts Health and Hospital Association has released a statement saying that “Primary care is our most powerful tool for building healthier communities, easing the burdens on emergency rooms and caregivers, and connecting patients with the personalized services they need. We commend state leaders for giving primary care the close attention it deserves.” However, they also caution that a spending target would need to “be implemented in a meaningful, pragmatic, and collaborative manner – especially within the context of the growing pressures and current investments that exist within today’s delivery system.”
As well, MassHealth, the state’s combined Medicaid and CHIP program, introduced primary care subcapitation for providers participating in MassHealth’s Accountable Care Organizations. This has increased investment in primary care[10] and is an example of how states can use Medicaid in strategies to better fund primary care.
In addition to efforts to advance primary care investment in Massachusetts, a recent analysis of the eight largest provider organizations in Massachusetts found that provider organizations with high primary care investment as a percent of total spending performed significantly better on standardized measures than those with lower primary care investments as shown below.
Primary Care Spending and Quality in Massachusetts
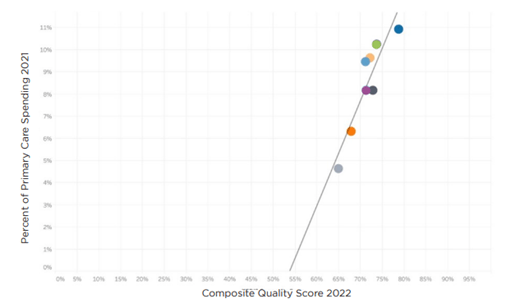
Note: The linear regression produced an R-squared value of .84 and a P-value of .001
Source: Analysis of Massachusetts: Primary Care Investment and Quality, Freedman Healthcare, July 2024
The study also assessed the relationship between spending on primary care and hospital spending for the eight organizations and found that those with higher investment in primary care experienced lower hospital spending as shown below. Though the predictive values were lower than in the quality analysis above, the findings illustrate the potential for primary care to stem avoidable inpatient care and emergency room visits.
Primary Care and Hospital Spending in Massachusetts
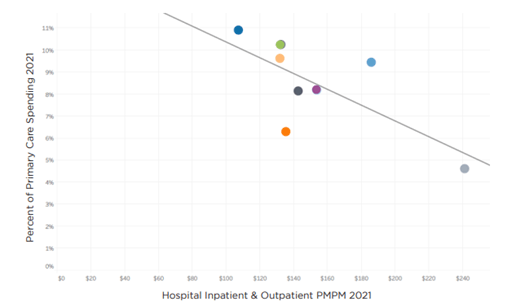
The linear regression produced an R-squared value of .50 and a P-value of .05
Source: Analysis of Massachusetts: Primary Care Investment and Quality, Freedman Healthcare, July 2024
- New Jersey requires Medicaid Managed Care Organizations to report the percentage of total medical expenditures devoted to primary care, as well as the State Department of Pension and Benefits to report on primary care spending for state-run health plans, such as the state employees’ plan. Though there is no statuary primary care spending target, a 2021 executive order set benchmarks for limiting overall health care cost growth, with targets of 3.2% for 2024 and 3.0% for 2025. The 2026 HealthCare Cost Growth Benchmark Report released in January 2026 by the state shows that statewide per person per year total health care expenditures increased by 6.1% between 2022 and 2023, exceeding the cost growth benchmark target of 3.5 % by 2.6 %. The report also includes per person spending by submarket for primary care spending, which shows a small increase from 2022 to 2023, the most recent data year available.
- In New York, Senate Bill S1634 would require health plans and payers to have a minimum of 12.5% of total medical expenditures on physical and mental health spending be spent on primary care services. The bill was introduced for the 2025-2026 legislative session, passed the New York State Senate, and is pending consideration by the State Assembly.
- North Carolina established a Primary Care Payment Reform Task Force (S. 259) in 2023 to define primary care, assess current spending and issue recommendations. The goal is to establish a primary care investment target, with the goal of increasing investment to improve health outcomes and control costs, following national trends for 12-15% benchmarks.
- Utah has a Primary Care Spend Project operated within the Utah Department of Health’s Office of Health Care Statistics, which uses all payer claims data to calculate the total amount of spending on primary care as a percent of total medical expenditures. The 2023 report shows CHIP primary care spending at 9.5% for 2022 using a narrow definition of primary care spending, and 6.2% for commercial payers.
- Vermont passed legislation in 2019 requiring the Green Mountain Care Board (GMCB) and the Department of Vermont Health Access (DVHA) to define primary care, measure spending, and develop methods to increase primary care investment, aiming for at least 12% of total healthcare spending, with goals to align Medicaid rates with Medicare, though there is not an enforcement mechanism. Additionally, the dissolution of a major health plan (OneCare Vermont) has challenged progress. Legislation has been introduced in the House and Senate however that is now under consideration that would set a target in state law that 15% of total health care spending in Vermont go to primary care, with the Vermont Medical Association encouraging passage.
There are four key lessons that can be drawn from the composite of efforts across the many states addressing increasing investment in primary care .
- Primary Care is In Crisis – The sheer quantity of states with initiatives to increase investment in primary care reflects concern about the primary care crisis nationwide. States are taking action to increase the percentage of spending that flows to primary care through legislation, rate review, state employee plan provisions and voluntary payer and purchaser-based initiatives to bolster the primary care infrastructure that patients depend upon.
- Definitions and Approaches Matter – The way that primary care investment is defined is important so that increased investment accomplishes better care for patients. Similarly, the approach and approach to increased investment help to orient provider behavior. There is merit in both the narrow definition of primary care spending (spending that flows to primary care physicians) so that team-based care can be resourced, but there is also merit in assessing the broader definition of primary care spending and the important roles that behavioral health and advanced practice providers play in whole-person care. It is also clear that Advanced Primary Care is gaining ground and will be the new north star for care delivery over time.
- Measurement Alone Doesn’t Do the Job – Measurement alone is important but insufficient. It is difficult to command attention and action to increase primary care investment without a penalty or consequence for non-compliance. Unsurprisingly, the data also illustrates that efforts with consequences for not meeting targets are the most effective at achieving the aim of increasing investment in primary care. Some states have financial penalties for health plans who do not meet incremental primary care target spending levels. Others require corrective action plans. Some use rate review as a way to enforce compliance with primary care spending targets. Products subject to rate review would be subject to meeting the incremental target for full approval.
- Increasing Investment in Primary Care is a Team Sport – In achieving a primary care spending target, employers, labor groups, trusts, and other purchasers are important stakeholders as state legislation applies only to fully-insured products and not to those who are self-insured and ERISA-exempt. However, self-insured groups can voluntarily replicate these provisions in their self-insured coverage designs, and leading purchasers across the nation have already started to incorporate increased investment in advanced primary care in their benefit designs.
- [1] Foubister V. Five States Leading Efforts to Increase Primary Care Spending. The Milbank Memorial Fund. March 12, 2025
- [2] https://www.americashealthrankings.org/explore/measures/Physical_distress/MI
- [3] https://www.chcf.org/wp-content/uploads/2022/04/InvestingPrimaryCareWhyItMattersCommercialCoverage.pdf
- [4] B. Starfield, et. al., Contribution of Primary Care to Health Systems and Health, Milbank Quarterly, 2005 Sep;83(3):457–502. doi: 10.1111/j.1468-0009.2005.00409.x
- [5] Implementing High-Quality Primary Care, National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on Implementing High-Quality Primary Care; Washington (DC): National Academies Press (US); 2021 May 4. ISBN-13: 978-0-309-68510-8ISBN-10: 0-309-68510-9
- [6] https://hcai.ca.gov/affordability/ohca/promote-high-value-system-performance/primary-care-investment-benchmark/
- [7] https://legis.delaware.gov/BillDetail/68714
- [8] https://dhss.delaware.gov/wp-content/uploads/sites/4/2025/02/pcrcstrategicplanrpt24.pdf
- [9] https://www.milbank.org/publications/states-lead-efforts-to-increase-primary-care-spending/#:~:text=OHIC%20also%20plans%20to%20implement,’%E2%80%9D
- [10] https://www.chcs.org/resource/massachusetts-primary-care-sub-capitation-model-implementing-primary-care-population-based-payment-in-medicaid/
